Medical Residency Surge: Balancing Quantity and Quality



STORY INLINE POST







 By Mauricio Gonzalez Urquijo | Full Time Faculty -
Mon, 01/19/2026 - 08:00
By Mauricio Gonzalez Urquijo | Full Time Faculty -
Mon, 01/19/2026 - 08:00
Over the past few years, Mexico has quietly carried out one of the largest expansions of medical residency positions in its history. On paper, this looks like a clear success: more training slots, more specialists, and a response to a long-standing shortage of doctors. But when we look beyond the numbers, an uncomfortable question emerges: Is the system growing fast enough to train specialists well, not just in greater quantity?
For decades, the National Medical Residency Exam (ENARM) was one of the tightest bottlenecks in Mexican medical education. Thousands of newly graduated doctors competed every year for a limited number of residency positions, often repeating the exam multiple times or abandoning specialist training altogether.
That has changed dramatically. In less than 10 years, residency positions have more than doubled. This expansion reflects an understandable policy goal: Mexico needs more specialists, and the system was clearly underproducing them. From a workforce perspective, increasing capacity was unavoidable.
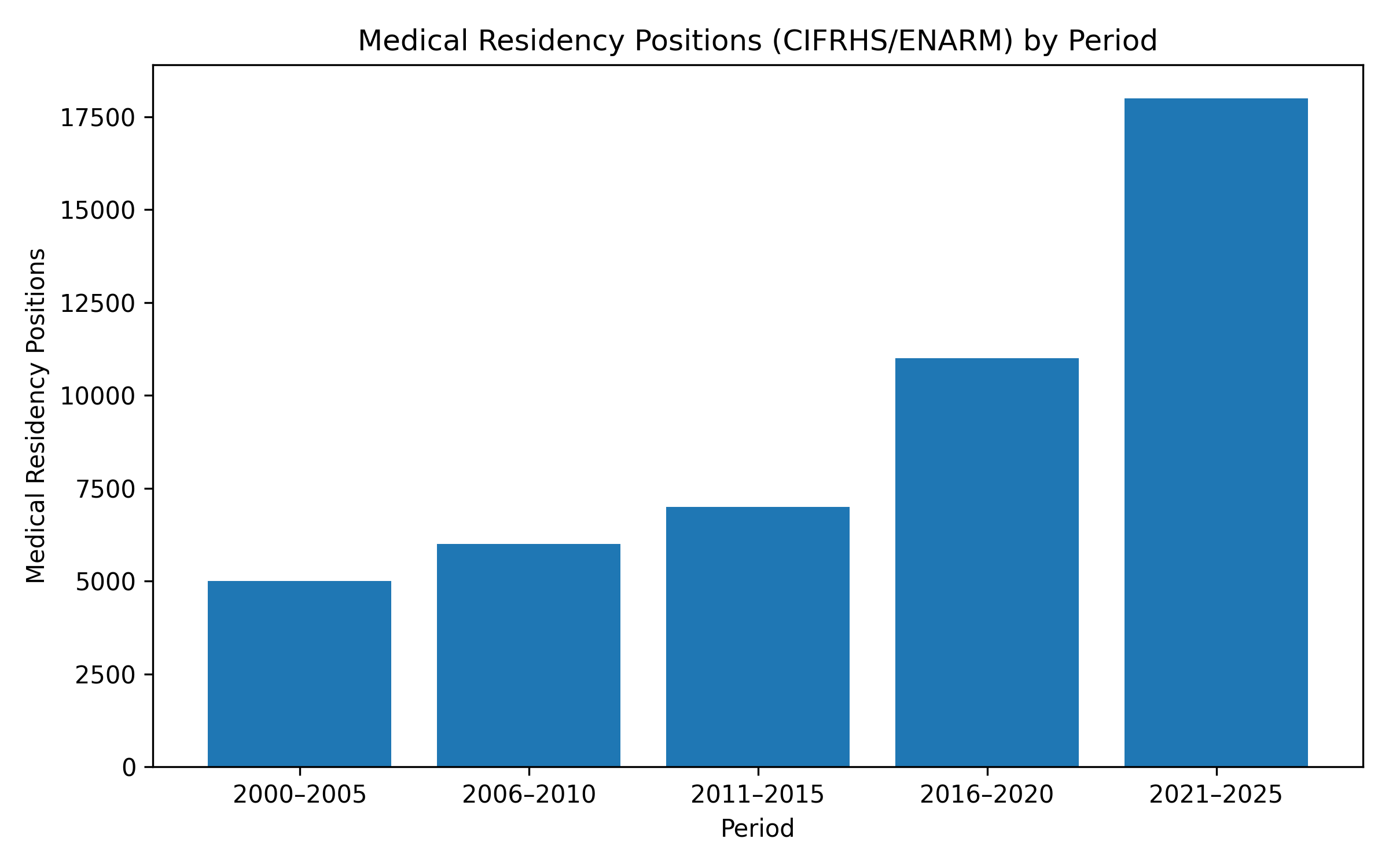
Figure. Medical residency positions in Mexico by period. Source: Author’s own elaboration based on publicly available CIFRHS/ENARM data. Values represent approximate period averages and are intended to illustrate long-term trends.
However, expansion alone does not guarantee better healthcare. While the number of residency positions has increased, training quality has not grown evenly across institutions or regions. Most top ENARM performers still concentrate in a small group of long-established teaching hospitals, while many newer or peripheral training sites struggle to attract candidates or offer comparable educational exposure. (1) This creates a paradox: There are more residency slots than ever before, yet access to complex cases, experienced mentors, and high-level hospitals remains limited for many residents.
Large public institutions illustrate this imbalance clearly. Although training sites have expanded rapidly across the country, the majority of residents still train in primary or secondary care units, with only a small proportion exposed to tertiary-level centers where highly complex medicine is practiced. (2) Quantity has increased faster than educational depth.
Residency training is not just an academic issue. Poorly aligned training systems have real-world consequences, to name a few:
- Patient safety suffers when supervision is limited.
- Health system efficiency declines when specialists are unevenly prepared.
- Legal and financial risks increase for institutions operating without strong educational oversight.
- Public trust erodes when expansion is perceived as lowering standards.
In other words, how specialists are trained ultimately affects everyone: patients, hospitals, insurers, and policymakers.
Recent changes to the ENARM process have made placement more flexible for applicants, but the new system relies almost entirely on exam scores to assign residency positions. Nowadays, programs have little or no say in selecting candidates who fit their clinical focus, teaching capacity, or institutional mission. (3)
Other countries faced this problem decades ago. In the United States and Canada, centralized matching systems were created to replace chaotic and inequitable recruitment. These models allow both applicants and residency programs to rank their preferences, producing better alignment and greater transparency. Mexico does not need to copy these systems blindly, but the principle of mutual selection is worth serious consideration.
If Mexico wants this expansion to succeed long term, the next phase of reform must focus on quality governance:
- Clear accreditation standards for all training sites
- Public reporting of program outcomes
- Ongoing evaluation of supervision, infrastructure, and educational results
Simply adding more positions without reinforcing these mechanisms risks diluting the very competencies residency training is meant to develop.
Equally important is strengthening undergraduate medical education. Persistent disparities in ENARM performance reflect uneven preparation long before residency begins. (1) Improving medical school accreditation, faculty development, and clinical exposure is essential if expansion is to translate into better healthcare rather than broader inequality.
Mexico’s rapid expansion of residency positions is a milestone worth acknowledging, but the true measure of success will not be how many specialists are trained, it will be how well they are trained. Balancing access, quality, and accountability is harder than increasing numbers, but it is the only way to ensure that today’s growth strengthens, rather than strains, the foundations of medical practice and public trust in the health system.
Mexico stands at a defining crossroads in medical education. The country has proven that it can expand residency positions at an unprecedented scale; what remains uncertain is whether it is willing to govern that expansion with the same ambition. Training specialists is not an administrative exercise, it is a long-term investment in patient safety, institutional credibility, and national health security.
If growth continues without robust accreditation, transparent outcomes, and meaningful alignment between residents and training programs, the system risks producing volume without value. But if this moment is used to strengthen supervision, modernize selection mechanisms, and hold institutions accountable for educational quality, Mexico could emerge with one of the most resilient and equitable residency systems in the region.
The ENARM should no longer be seen as an endpoint, but as the beginning of a broader, smarter process , one that places educational integrity on equal footing with access. Policymakers, academic leaders, and healthcare institutions now face a choice: manage residency training as a short-term response to workforce shortages, or design it as a strategic pillar of national development.
The opportunity is still open. The decisions made today will shape not only the next generation of specialists, but the future trust of patients in Mexico’s healthcare system.
Sources:
- Gaxiola-García MA, Villalpando-Casas J de J, García-Saisó S, García-Minjares M, Martínez-González A. National examination for medical residency admission: academic variables and performance among different schools. Salud Publica Mex. 2020;63,60-67. doi:10.21149/11576
- IMSS Grows Residency Program; Challenges Persist. https://mexicobusiness.news/health/news/imss-grows-residency-program-challenges-persist. Access on November 9, 2025
- Comision Interinstitucional para la Formacion de Recursos Humanos para la Salud. https://cifrhs.salud.gob.mx. Access on November 9, 2025
You May Like







Most popular







